delta dental application form
OF DENTAL INSURANCE form below and e-mail the completed form to. Delta Dental of New Jersey.
2
Broker Information Change Request.
. Delta Dental of New Mexico. 100 Sun Avenue NE Suite 400. Tips to avoid processing delays 1.
Locum Tenens Provider Form. DDIP1-001 9142020 Thank you for enrolling in your Delta Dental Individual and Family plan. Ad Protect your smile prevent tooth loss.
Dental Wellness Plan Application - DWP Agreement. Required fields are starred and must be completed to ensure enrollment. Dentist Directory Update Form.
EnrollmentChange of Status Forms for GroupEmployer EnrollmentChange of Status Form for GroupEmployer Dental Policy EnrollmentChange of Status Form for GroupEmployer Dental Policy Spanish version. Dentist Administrative Forms and Resources. Continuous Orthodontic Coverage Form for DeltaCare USA.
PO Box 40384 Portland Oregon 97240-0384 Dental plans in Oregon provided by Oregon Dental Service dba Delta Dental Plan of Oregon. Coordination of Benefits pdf 1 page The coordination of benefits form helps Delta Dental to determine which plan if not the sole plan has the primary payment. Box 981400 Boston Massachusetts 02298-1400 Please print or type.
If your form is received after the. Save up to 35 off standard dental rates today. Large Group Master Application Form PPO Maximum Wellness 2022.
Dental Forms Small Groups Fewer than 100 employees Small group subscriber enrollmentchange form. Delta Dental Master Application. Adults and parents of children ages 12 and younger illuminate what they thought about their oral health and what they did to properly care for it at home and with their dentist during 2021.
Employer Toolkit Access Request Form. DeltaVision HIPAA Form 14a Risk Groups. While many adults are unaware of how oral health and overall health are connected most.
Large Groups 100 employees. Dental plans in Alaska provided by Delta Dental of Alaska 60403711 120 Section 1. Ad Enroll in a dental insurance plan with Guardian Direct get covered.
Do not use another providers application. Mail this form to Delta Dental Mail. Whether youd like to modify your current plan or apply for new benefits youll find the tools to do so below.
Small Groups 2-150 eligible employees Small Group Application with Dental and Vision. Thats why most dentists choose to work with Delta Dental to protect their patients smiles. SECTION 1 Provider Type Name.
Delta Dental PPO and Delta Dental Premier network dentists submit claim forms automatically on behalf of Delta Dental patients. This form is not needed for orthodontic referrals. Complete only this application and its supplemental forms.
Little Rock AR 72231. For more information on becoming a network dentist enter the. Issued by Delta Dental you must sign and return this form with your application.
Find a Vision Provider. I select the following dental plan for the requested effective date of. Enrollment Form DeltaCare English 2022.
Delta Dental Premier Network Forms - Professional Application. Mail completed claims to. Get the most out of your companys Delta Dental benefits.
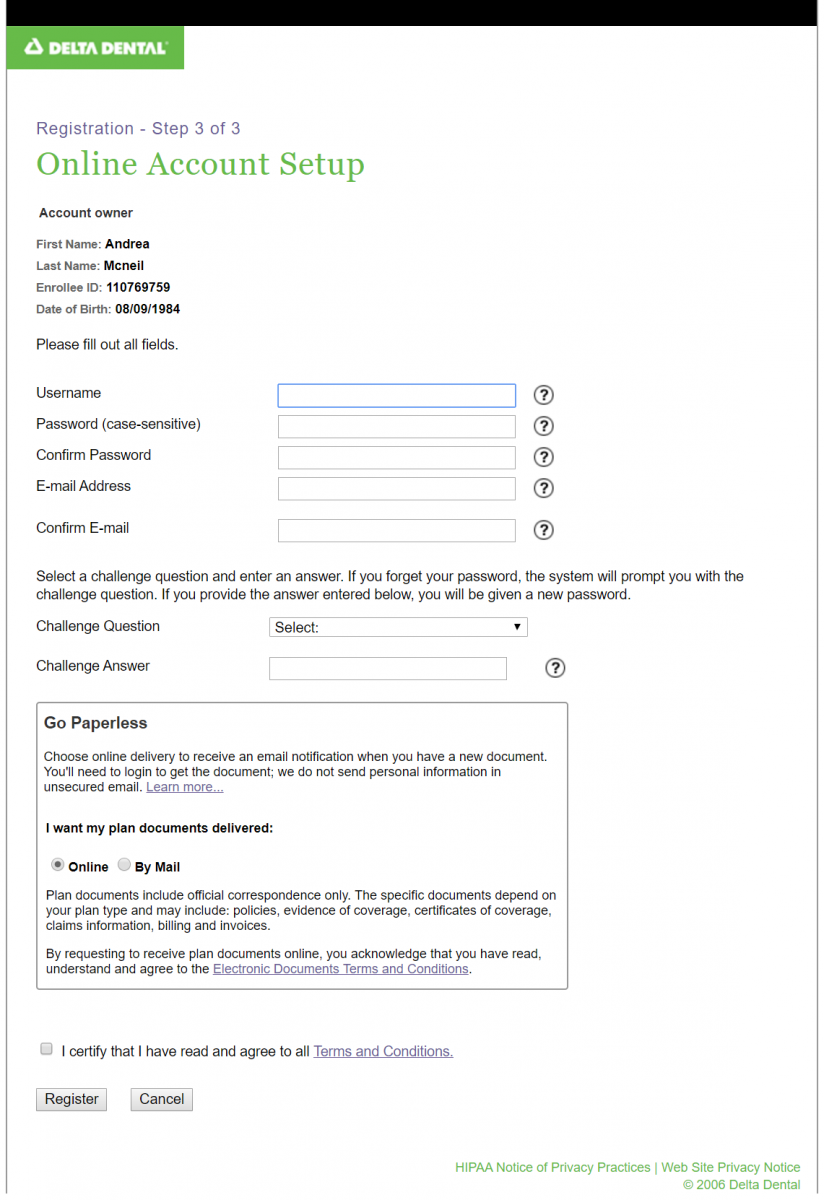
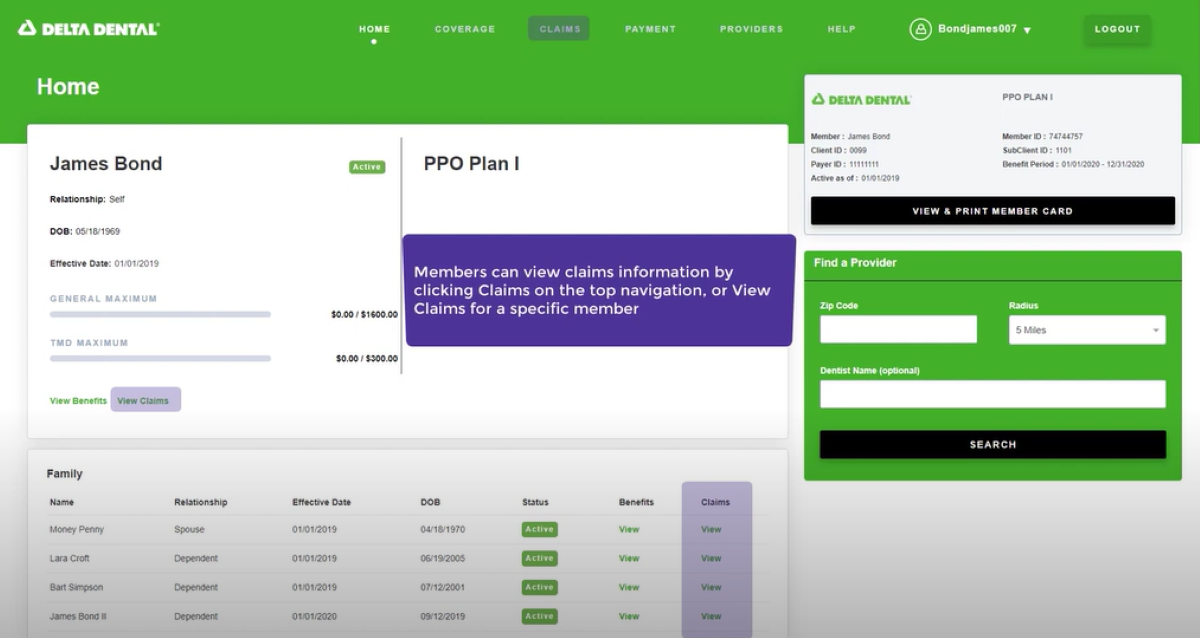
ND Master Application for Health Care Reform Certified Group Products. To access a dental claim form enrollees can log into Member Portal. Join our dentist network.
For your own information and protection certain facts should be pointed out to you which could affect your rights to coverage under the new policy. Use this form to update the status of your practice as a DeltaCare provider. PDF forms may be downloaded.
Website authorization form for pool-rated groups. Hawki Orthodontic Network Forms - Hawki Orthodontic Agreement. Application and Change Form for Individual Family Dental Insurance PO.
303-741-4233 It is agreed that the Group Contract will not become effective unlessuntil this application is approved and accepted by Delta Dental of Colorado. Large Group Master Application Form Premier 2022. Download Insurance Forms Information.
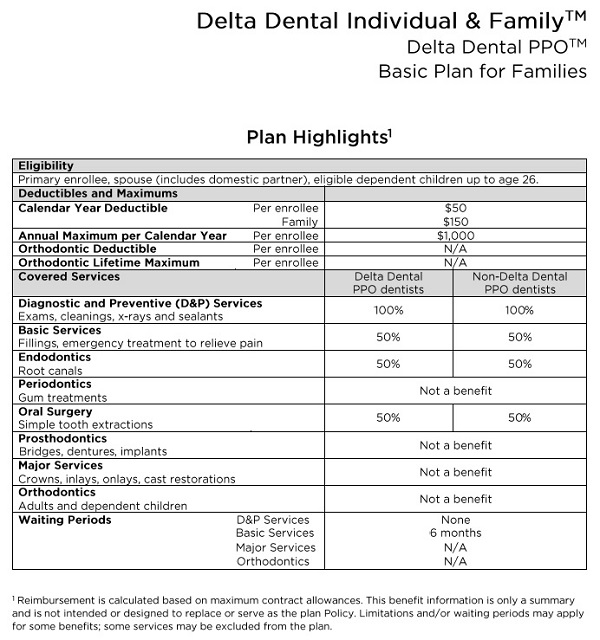
Use this form to file a claim for services performed in the United States. Please note that your enrollment form and payment must be received on or before the 25th of the month for coverage to start the first of the following month. Delta Dental Individual and FamilyTM.
Enrollment and Maintenance Forms. Removable Prosthodontics Assessment Form. Subscriber must be age 18 or older.
Group Claim Form This claim form is for Delta Dental PPO Delta Dental Premier and non-network claims. We cover more Americans than any other dental benefits provider - and strive to make dental coverage more accessible and affordable to a wide variety of employers groups and individuals. Delta Dental PPO participation packet request.
HIPAA Form 14a Risk Groups. Group Master Application DeltaCare 2022. MNND Eligibility EnrollmentUpdate Form.
Delta Dental of Colorado Sales and Marketing Email Address. Find a Dental Provider. Small group employee enrollment form.
Please mail your claim form to. Automatic Draft Authorization Form Employee Enrollment Form English Employee Enrollment Form Spanish Onetime Load Enrollment Template General Change Form for Groups editable. Delta Dental of Wisconsin.
Direct Debit Authorization ACH Form. Dental AgencyAgent Data Request. HIPAA Form 14b ASO Groups.
Ƨ TMDelta Dental PPO 1000 annual maximum plan payment limit Ƨ Delta Dental EPOTM 1500 annual maximum plan payment limit Ƨ TMDelta Dental PPO Bright Smiles No annual maximum plan payment limit All dental plans have 0 deductible. DeltaVision HIPAA Form 14b ASO Groups. MN Membership Enrollment Form Spanish Small Group Pooled MN ND Enrollment Form for Health Care Reform Certified Group.
Let Delta Dental help our more than 80 million members find their way to your office. Large Group Master Application Form PPO 2022. Enrollment Department Delta Dental of Massachusetts PO Box 9695 Boston MA 02114-9695 Please note that your coverage will NOT be in effect until we receive the completed and.
Delta Dental PPO Network Forms - Delta Dental PPO Supplemental Agreement. More Americans choose Delta Dental than any other dental insurance provider. Dental Initial Credentialing Application Ready to submit.
Enrollment Form Small Group English 2022. Group Application with Dental and Vision. Optional Treatment Consent Form Use this form if your patient elects to have optional treatment completed.
Choose the right plan to keep you smiling. DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist. Practitioner and practice information.
Find the forms and resources to assist you in administering Delta Dental of Oklahoma benefit products and services. Group Master Application Small Group 2022. Delta Dental Individual and Family.
Ulster Street Suite 800 Denver CO 80237 Fax Number. Do not use nicknames or initials unless they are part of your legal name. Findings from the Delta Dental-commissioned research of 2000 US.
Delta Dental is Americas largest and most trusted dental benefits carrier. You can download this form insert the necessary information and print it or you can print it and fill in the applicable information. DeltaCare USA participation packet request.
Health conditions which you may presently have may not be covered under the new policy.

Using Udp
Dental Insurance

Forms And Resources Delta Dental Of Michigan
Member Forms Documents Delta Dental Of Arizona
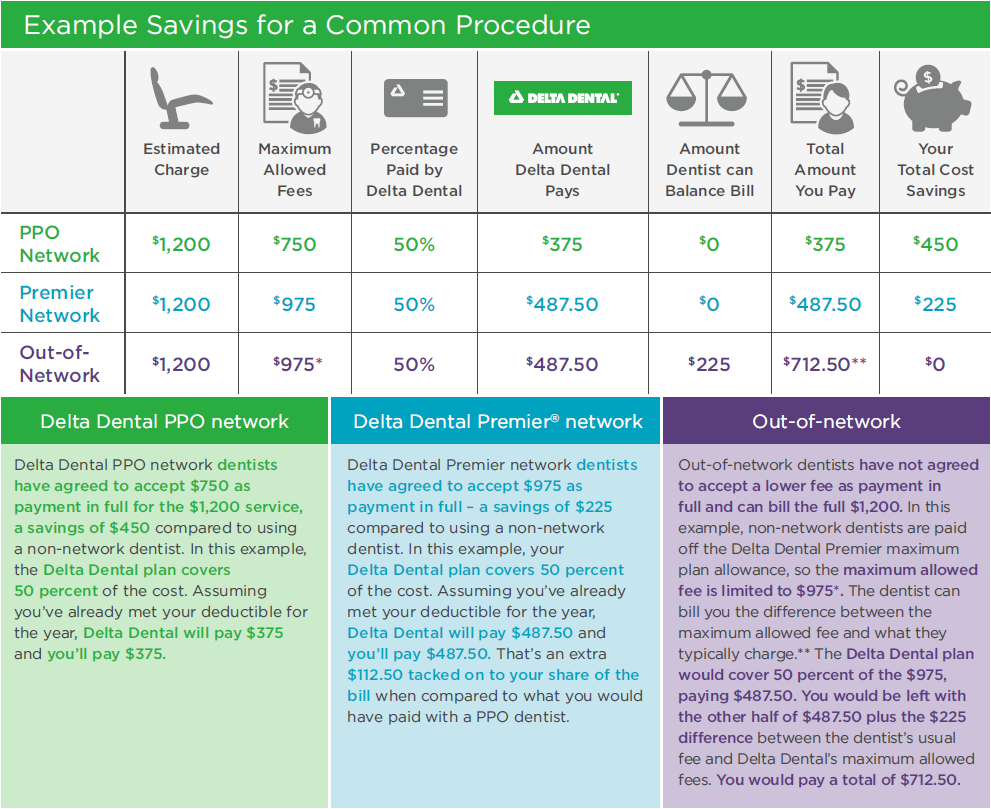
Ppo Vs Premier Dental Coverage Delta Dental Of Illinois

Dentist Connection Delta Dental Of Iowa
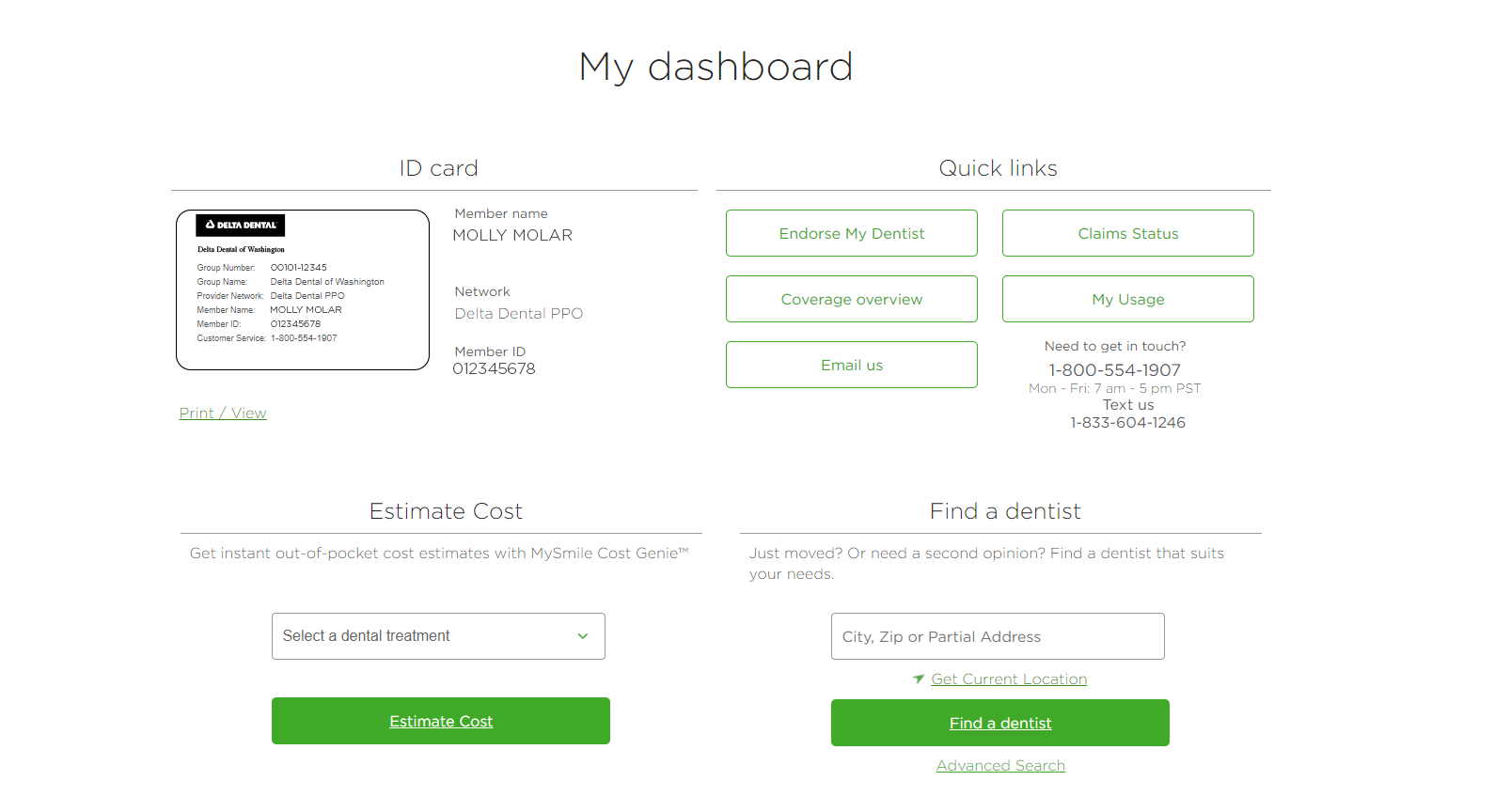
Dental Benefits Guide How To Check The Status Of Your Dental Claim Delta Dental Of Washington
2
Dentist Forms Documents Delta Dental Of Arizona
![]()
Delta Dental

Delta Dental Member Faq
Employer Forms Resources Delta Dental Of Ohio
![]()
Join Delta Dental Dentist Network
Delta Dental Individual Family Plans For 2019

Claim And Admin Forms Delta Dental
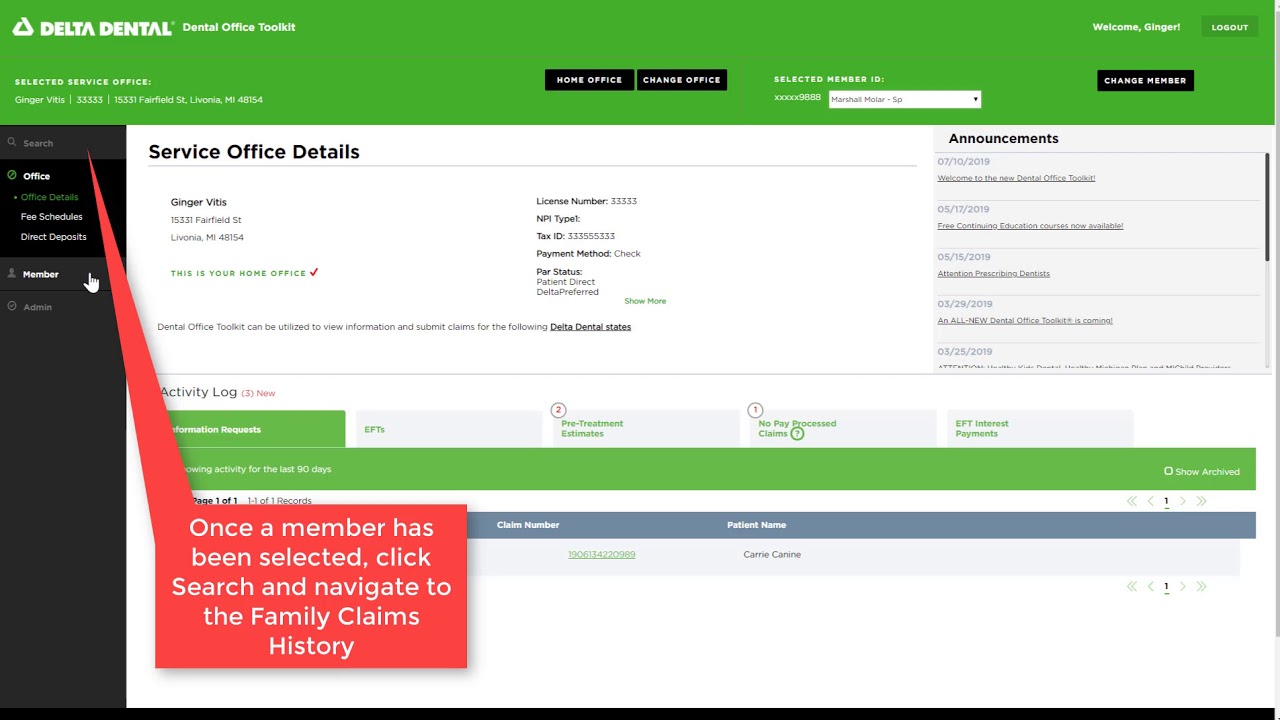
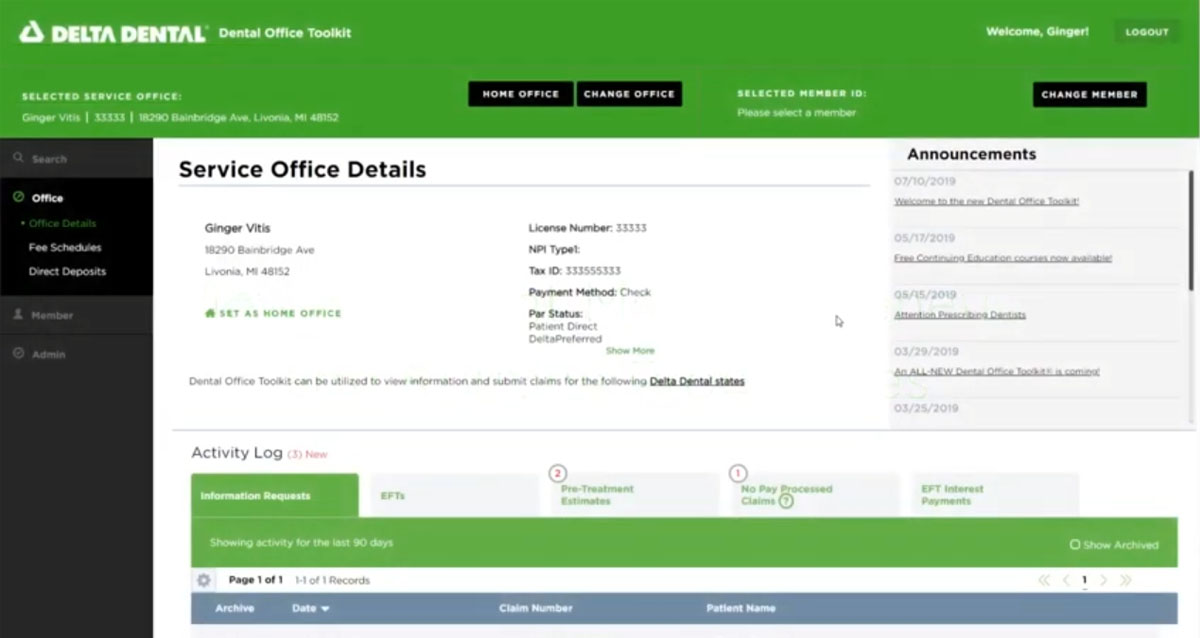
Dental Office Toolkit Delta Dental Of Ohio

Delta Dental 101
Member Resources Delta Dental
Member Forms Documents Delta Dental Of Arizona